
Integrating experiential learning theory with innovation and entrepreneurship education: a qualitative study on Chinese medical students | BMC Medical Education

Integration of ELT with IEE: A theoretically grounded framework for medical students’ entrepreneurial development
The integration of Experiential Learning Theory (ELT) with Innovation and Entrepreneurship Education (IEE) constructs an adapted theoretical framework for fostering medical students’ entrepreneurial and innovative capabilities. This study expands the application of ELT by tailoring it to the context of medical entrepreneurship, which fills a critical gap in the IEE literature: It addresses the shortage of theoretical analysis focusing on students’ learning experiences. While previous research has applied ELT to general entrepreneurship education [47, 48], our framework uniquely addresses the inherent tensions between evidence-based medical training and entrepreneurial skill development, thereby providing a more targeted and practical theoretical support for cultivating medical students’ innovative and entrepreneurial competencies.
This theoretical contribution is significant because medical students face unique epistemological challenges when transitioning between clinical reasoning (which prioritizes evidence, protocols, and risk minimization) and entrepreneurial thinking (which embraces uncertainty, ambiguity, experimentation, and calculated risk-taking). Our findings reveal that students with prior entrepreneurial exposure (31.4% of our sample) demonstrated enhanced resilience during initial uncertainty phases, while those without such background experienced profound disorientation.
Our adapted framework provides a structured approach to navigate these contradictions through four interconnected stages: Concrete Experience (CE), Reflective Observation (RO), Abstract Conceptualization (AC), and Active Experimentation (AE). This reconceptualization addresses a theoretical gap identified by Morris et al. [49], who argue that entrepreneurship education often lacks clear theoretical foundations specific to disciplinary contexts. Our model provides robust theoretical justification for how medical students develop entrepreneurial competencies while navigating the unique constraints and opportunities within healthcare systems.
How ELT facilitates innovation skills development in medical context
Our adapted framework provides a structured approach to navigate the dynamics between clinical and entrepreneurial thinking through the ELT four-stage cyclical model, connected by the transitional processes of reflect, synthesize, apply, and iterate (see Fig. 2).
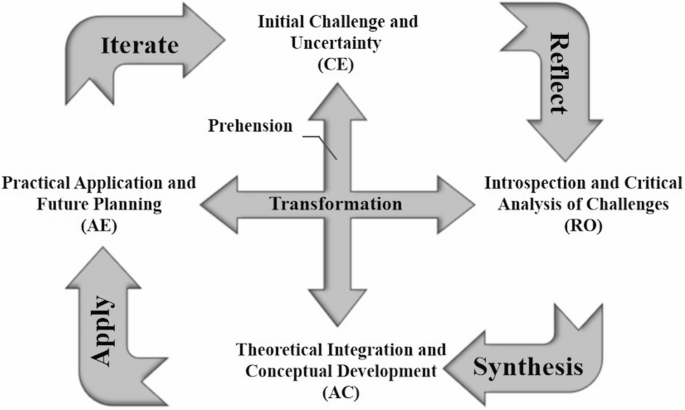
The ELT learning circle embedded in IEE
(1) Reflect: Concrete Experience → Reflective Observation
Medical students’ entrepreneurial learning begins with encountering three unique forms of uncertainty: technical uncertainty (unfamiliarity with business concepts and innovation processes), market uncertainty (unclear understanding of healthcare market dynamics and value creation), and outcome uncertainty (difficulty reconciling clinician and entrepreneur roles). These uncertainties create disorientation that becomes the catalyst for deep learning, which posits that disorienting dilemmas or concrete experiences initiate the learning cycle. In this context, the ambiguity of entrepreneurship serves as a critical divergence from the structured certainty of clinical routines, compelling learners to confront and adapt to a new domain.
Unlike general entrepreneurship students who may approach innovation primarily through market opportunity recognition [50], medical students demonstrate systems-oriented reflection—their concerns extend beyond immediate project challenges to encompass broader healthcare system implications, regulatory frameworks, and ethical considerations. This finding extends ELT literature by demonstrating how disciplinary background fundamentally shapes the nature of concrete experiences and subsequent learning processes [46]. Specifically, this integrative epistemological frame, shaped by prior socialization in high-stakes clinical settings, underpins medical students’ systems-oriented thinking and influences how they engage with complexity, collaboration, and identity within healthcare environments [51, 52].
The transition to Reflective Observation is marked by students’ ability to transform initial discomfort into structured introspection. One student (N28, 21-year-old female, Physical Therapy, third-year undergraduate student) illustrated this transformation: “Initially, I was completely unaware of what entrepreneurship and innovation entailed, as well as how to draft a business plan. Through repeated presentations, I was able to reflect on the questions posed by teachers and peers, respond accordingly, and thereby enhance the project’s [Brain-Computer Interface Upper Limb Rehabilitation Robot] quality.” This reflection process diverges markedly from clinical reflection, which typically focuses on diagnostic accuracy or treatment outcomes. In entrepreneurial contexts, students must reflect on ambiguous problems with multiple valid solutions, which demonstrates an epistemological shift that challenges their evidence-based training. This aligns with Kolb’s notion of learning as a process where knowledge is created through the transformation of experience, particularly when learners are pushed to reinterpret familiar epistemological schemas [29, 53].
(2) Synthesize: Reflective Observation → Abstract Conceptualization
The synthesis phase represents the most challenging transition in the learning cycle, with our findings revealing substantial difficulty among medical students in transitioning from specific observational data to general entrepreneurial principles. This difficulty stems from the need to integrate two fundamentally different epistemological frameworks: medical knowledge (emphasizing evidence, standardization, and risk minimization) and entrepreneurial knowledge (emphasizing opportunity recognition, innovation, and calculated risk-taking). Kolb [29] underscores this as a shift from Reflective Observation to Abstract Conceptualization, wherein learners construct theoretical insights from practical reflection. However, as Boon and Van Baalen [54] notes, professional knowledge is often tacit and domain-specific, creating friction when learners confront cross-disciplinary integration.
A pediatric project leader (N29, 21-year-old male, Occupational Therapy, third-year undergraduate student) exemplified successful synthesis: “Our project [Eye-Tracking-Based Screening System for Children with Autism] faced significant setbacks due to data loss, almost leading us to give up while managing our rigorous academic workload. Under our mentor’s guidance, we persevered and devised an innovative approach for autism screening in children based on eye-tracking technology.” This case demonstrates how synthesis involves not just combining knowledge domains but transforming setbacks into opportunities for innovation, which demonstrates a process Politis [55] identifies as entrepreneurial learning through prior failure and reflection.
The challenge of synthesis is compounded by epistemological friction, the resistanceencountered when attempting to merge different ways of knowing [54]. Medical Medicalstudents must learn to value uncertainty and ambiguity as sources of opportunity rather than problems to be eliminated, fundamentally challenging their clinical training. As Billett [56] emphasizes, learning across boundaries requires the negotiation of meaning meaning between culturally and epistemologically distinct practices. This finding suggests that effective entrepreneurship education for medical students requires explicit attention to epistemological differences rather than assuming students can naturally integrate different knowledge systems.
(3) Apply: Abstract Conceptualization → Active Experimentation
The application phase proved challenging, with our findings revealing that medical students face unique difficulties in transitioning from conceptual models to active experimentation. This challenge reflects the unique demands of medical entrepreneurship, which requires simultaneous clinical and market validation—a dual imperative that significantly complicates implementation compared to general entrepreneurship education. In Kolb’s model, this shift corresponds to Active Experimentation, where learners test new ideas in the real world.
A doctoral student (N34, 30-year-old male, Rehabilitation Medicine [Integrated Chinese & Western Medicine], third-year Ph.D. candidate) described his approach to developing an upper limb rehabilitation robot: “Initially, we conducted clinical studies to identify established movement patterns. These were synthesized into a standardized training protocol, which we mechanized using modern technology. When initial market feedback highlighted cost barriers, we reengineered the system to prioritize affordability without compromising clinical efficacy.” This example illustrates how successful application requires continuous navigation between clinical requirements and market constraints, which can be seen as a complex optimization process that extends traditional ELT assumptions about linear progression from concept to application.
Furthermore, as Mezirow [33] explains in Transformative Learning Theory, application becomes a site of transformation when individuals reframe their assumptions through active problem-solving. The application phase also revealed the critical importance of institutional support. Students in programs with established industry partnerships demonstrated significantly higher success rates in transitioning to active experimentation.
(4) Iterate: Active Experimentation → Concrete Experience
Our findings suggest significant institutional and temporal constraints on iterative learning, with important implications for program design, as incomplete cycles may limit the development of entrepreneurial resilience and adaptive capacity. Students who successfully engaged in iteration described processes of continuous refinement based on multiple forms of feedback. One participant (N6) noted: “Upon discovering discrepancies between project [Wrist-Ankle Acupuncture Device for Dysmenorrhea Treatment] content and competition criteria, we engaged in deep reflection based on expert feedback and made every effort to correct these issues, often amending our business plans over a hundred times. A spirit of perseverance and a clear direction of effort are crucial for overcoming challenges in medical innovation.”
This iterative process in medical entrepreneurship differs significantly from other fields due to healthcare’s complex regulatory environment, ethical considerations, and extended validation timelines. According to Kolb & Kolb [46], experiential learning spaces must support recursive engagement, allowing learners to cycle repeatedly through experience, reflection, and adaptation. This process builds adaptive expertise [57] by encouraging learners to apply knowledge flexibly across varied contexts, which is crucial in domains like medicine and entrepreneurship, where knowledge must be continually reshaped to meet new challenges.
(5) Concrete Experience ↔ Abstract Conceptualization: Reflect to Synthesize
Kolb’s model extends beyond sequential stages to include two critical dimensions (i.e., prehension and transformation) that enrich the learning process in IEE contexts. The prehension dimension between Concrete Experience and Abstract Conceptualization underscores the process of reflecting on real-world experiences to synthesize theoretical insights. This dimension is particularly salient in IEE, as students grapple with unfamiliar challenges such as business model development, market feasibility analysis, and healthcare innovation. For instance, designing a novel healthcare device may compel students to develop a framework that integrates clinical efficacy with market sustainability.
Such integrative synthesis aligns with recursive process of professional learning anchored in the construction of knowledge through practice, enabling the conceptual transfer of capacities across domains. It ensures that theoretical constructs are not only grounded in experiential knowledge but also directly applicable to practical scenarios, fulfilling Kolb’s premise that learning is the process whereby knowledge is created through the transformation of experience.
(6) Active Experimentation ↔ Reflective Observation: Apply to Iterate
The transformation dimension between Active Experimentation and Reflective Observation highlights the iterative cycle of applying knowledge and refining strategies based on reflective feedback. This interplay allows students to critically evaluate the outcomes of their entrepreneurial efforts. A student (N18, 23-year-old male, Rehabilitation Medicine and Physiotherapy, first-year Master student) mentioned that when confronted with abstract issues, he tends to utilize AI tools to enhance situational awareness. By employing this method, he is able to assess the correctness of existing solutions. Ultimately, he continually iterates and refines his innovative proposals through practice. This dynamic exemplifies how Kolb’s experiential learning cycle, through recursive engagement with abstract conceptualization and active experimentation, generates novel epistemological frameworks essential for entrepreneurship, that is, transcending adaptive responses to create new possibilities.
Barriers to effective ELT integration in IEE
Institutional and resource constraints
Despite the benefits of IEE, medical students face several constraints that impact their entrepreneurial endeavors. These constraints disrupt different stages of the learning cycle, hampering the development of entrepreneurial competencies.
Venture capital and resource availability represent primary limitations that disproportionately affect the Concrete Experience and Active Experimentation phases. As noted by a student (N28, 21-year-old female, Physical Therapy, third-year undergraduate student), medical students often lack access to the technical resources and expertise needed to develop and implement innovative solutions: “Even with a brilliant medical concept, we couldn’t proceed past basic prototyping because specialized fabrication equipment wasn’t available. We had to modify our entire approach to work with available resources, which compromised the potential clinical impact of our solution.” This statement reveals how resource constraints fundamentally alter the learning experience—students learn to compromise innovation for feasibility rather than pursuing optimal solutions. This creates a bifurcated learning process where some students develop workarounds that enhance creative problem-solving, while others become frustrated and disengage from entrepreneurial activities altogether. Additionally, students are often forced to rely on external collaborators for technical skills and financial support, which underscores the need for better resource allocation and support structures within medical schools.
Technical capabilities, particularly expertise in computer technology and marketing, also pose significant challenges that interrupt the Abstract Conceptualization and Active Experimentation phases of ELT. As a participant (N2, 20-year-old male, Physical Therapy, third-year undergraduate student) described: “We needed motion tracking algorithms not available within our medical school. Without technical partners, we spent months trying to develop skills that engineering students acquire in their first year.” This gap between medical training and technical requirements makes students struggle to integrate technical components into their entrepreneurial frameworks. This extends Kolb’s theory by demonstrating how domain-specific knowledge gaps can hinder learning cycles.
Financial support and project guidance are critical factors that influence all phases of the ELT cycle in medical entrepreneurship education. “With sufficient funding, we could have conducted proper market validation studies rather than relying on convenience samples. Our learning was compromised because we couldn’t test assumptions with real stakeholders.” (N24, 21-year-old male, Physical Therapy, fourth-year undergraduate student) This quote illustrates how financial constraints limit not just implementation but the very ability to learn through Active Experimentation.
Market and Policy Environment factors also play a role in constraining entrepreneurial activities. Government policies, such as those related to COVID-19, and the overall suitability of the market for new ventures are significant challenges. In terms of Concrete Experience, students must navigate a complex landscape of regulations and market conditions. Reflective Observation in this context involves evaluating how these externalities limit the scope of their projects, often leading to a reconsideration of ideas or a scaling back of ambitious goals. As students move to Active Experimentation, regulatory and market constraints limit their ability to fully test ideas in a real-world context. Advocacy for more supportive policies and a favorable entrepreneurial climate could mitigate these constraints.
Implications for medical education reform
The integration of ELT into medical entrepreneurship education holds significant implications for broader medical education reform. As Kolb emphasized, effective learning requires not just experience, but the active transformation of that experience into concepts and action [29]. Our findings suggest that effective entrepreneurship education requires fundamental reconsideration of how medical students learn, that is, moving from knowledge acquisition to knowledge application and creation.
A key implication emerges from our analysis: effective entrepreneurship education requires faculty to serve as mentors and connectors rather than solely as content experts. One IEE supervisor reflected that teaching entrepreneurship to medical students prompted a fundamental shift in their teaching approach. Rather than acting as an authority figure, they assumed the role of a guide, supporting students as they navigated uncertainty. This aligns with the facilitative role of educators in experiential learning as emphasized by Kolb & Kolb [46].
Such reflections highlight how entrepreneurship education can catalyze broader pedagogical reform in medical education, promoting experiential approaches that may better equip students to manage the complexities and uncertainties of modern medical practice.
Chinese context and global relevance
In contrast to many other countries, IEE in China is notable for its expansive scale and deep integration into higher education. Within the medical domain, IEE has been elevated as a strategic priority, positioning students at the intersection of interdisciplinary innovation and professional development. These opportunities align closely with Kolb’s ELT model, offering a structured cycle of experience, reflection, conceptualization, and experimentation that enriches medical education.
By recognizing IEE as one of the five core competencies for medical professionals, Chinese institutions highlight the role of experiential learning in bridging the gap between theoretical instruction and practical application. However, the ambitious scale of China’s IEE initiative also introduces epistemological and logistical burdens, particularly when entrepreneurial content lacks direct clinical connection. Moreover, the vast number of participants in IEE programs can dilute the quality of mentorship and individualized guidance, both of which are essential for meaningful Reflective Observation and Abstract Conceptualization. Without structured reflection and mentorship, students may cycle through experiences without achieving deep learning.
To optimize the IEE experience, more discipline-specific programs are required, which bridge entrepreneurial learning with clinical realities. These should emphasize the Reflective Observation and Abstract Conceptualization stages of ELT, enabling students to develop nuanced understandings of how innovation principles apply in healthcare. Additionally, personalized mentorship is equally critical. ELT posits that transformation of experience into knowledge is greatly facilitated by skilled facilitation [46]. With dedicated mentorship, students can more confidently navigate innovation in healthcare and cultivate the integrative thinking essential for modern medical practice.
Globally, China’s experience offers valuable lessons. As healthcare systems grapple with rapid change and uncertainty, integrating IEE offers a promising strategy to prepare clinicians who are both technically proficient and adaptively innovative. China’s systematic approach, while not without challenges, exemplifies how national policy, curriculum integration, and experiential principles can be aligned to embed entrepreneurial thinking in professional training.
link






